The Office of Inspector General (OIG) of the Department of Veterans Affairs conducted a review to assess a safety concern with the new electronic health record (EHR) that resulted in patient harm. The OIG found that the new EHR sent thousands of orders for medical care to an undetectable location, or unknown queue, instead of to the intended location. Veterans Health Administration (VHA) identified and ranked safety concerns with the new EHR. In
December 2021, VHA assessed the risk of the unknown queue as “major severity,” “frequently occurring,” and “very difficult to detect.” As such VHA recognized immediate mitigation was needed. Oracle Cerner failed to inform VA end-users of the existence of the unknown queue and put the burden on VHA to mitigate the problem.
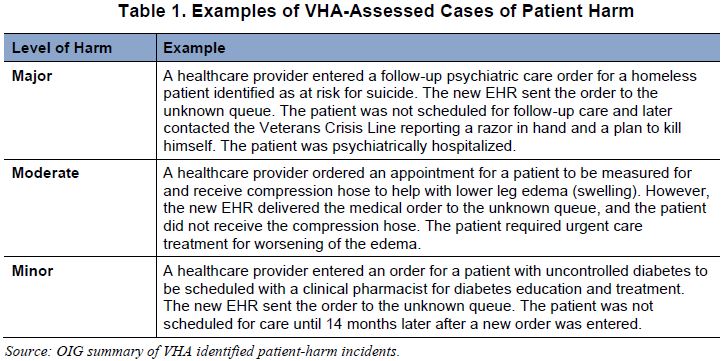
Beginning in June 2021, VHA staff spent substantial hours to complete clinical reviews to assess patient risk and harm related to the unknown queue and found that the new EHR’s delivery of orders to the unknown queue caused 149 patient harm events.
In late 2021, VHA staff provided the Deputy Secretary and the Executive Director for VA’s EHR modernization effort with information on the unknown queue safety concern and identified patient harm.
Each facility that goes live with the new EHR will require an ongoing commitment from facility staff to monitor and address the new EHR’s unknown queue. Cerner and VHA took actions to minimize orders being routed to the unknown queue. However, after finding over 200 orders in the unknown queue in May 2022, the OIG has concerns with the effectiveness of Cerner’s plan to mitigate the safety risk.